New U.S. Dietary Guidelines To Drop Cholesterol Limits
By James J. Kenney, PhD, FACNThe main goal of the 2015 U.S. Dietary Guidelines Advisory Committee (DGAC) report appears to move away from recommending any specific optimal diet or to focus primarily on specific nutrients but rather to help guide Americans to choosing an overall healthy dietary pattern. It is hard to argue with the DGAC's statement that a "healthy dietary pattern is higher in vegetables, fruits, whole grains, low- or nonfat dairy, seafood, legumes, and nuts; moderate in alcohol; lower in red and processed meats; and low in sugar-sweetened foods and drinks and refined grains." One might quibble with the suggestion that "low-fat" dairy products ought be included because many "low-fat" dairy products are still quite high in saturated fat and cholesterol. However, to its credit the DGAC report continues to recommend limits on the intake saturated fat, trans fat, and salt (sodium). The most obvious tragic flaw in an otherwise mostly science-based report was the Advisory Committee's questionable decision to no longer include any limit on dietary cholesterol intake.Despite all the media hype about the DGAC's most controversial decision, the report itself had surprisingly little to say about dietary cholesterol or why they decided to dump the long-standing dietary guideline for Americans to limit their intake of cholesterol (to no more than 300mg/day). This is all the DGAC's report had to say about that specific decision:"Cholesterol. Previously, the Dietary Guidelines for Americans recommended that cholesterol intake be limited to no more than 300 mg/day. The 2015 DGAC will not bring forward this recommendation because available evidence shows no appreciable relationship between consumption of dietary cholesterol and serum cholesterol, consistent with the conclusions of the AHA/ACC report. [2, 35] Cholesterol is not a nutrient of concern for overconsumption."So there on page 90 are the 4 lines explaining the DGAC's rationale for dumping any limits on cholesterol intake. Perhaps the two references cited provide convincing new scientific evidence that dietary cholesterol does not actually raise total-cholesterol and LDL-C or perhaps that higher levels of serum cholesterol are no longer believed to promote atherosclerosis and cardiovascular disease (CVD)? Let's take a closer look at those two references and see whether or not they really provide credible scientific support for dumping the long-standing US Dietary Guideline to limit dietary cholesterol:Reference #2: Eckel RH, Jakicic JM, Ard JD, de Jesus JM, Houston Miller N, Hubbard VS, et al. 2013 AHA/ACC guideline on lifestyle management to reduce cardiovascular risk: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation. 2014;129(25 Suppl 2):S76-99. PMID: 24222015. http://www.ncbi.nlm.nih.gov/pubmed/24222015.Well Eckel RH et. al. do conclude that the data they reviewed from observational studies that: "…there is insufficient evidence to conclude that lowering dietary cholesterol reduces the risk of CVD." Of course, nutrition researchers have long known data from observational studies often miss what is almost certainly a causal association between CVD and dietary components such as not only cholesterol, but also dietary salt and saturated fatty acid (SFA) and CVD. One well-known problem with observational data is that it can easily miss a real causal association due to a very inaccurate assessment of people's dietary cholesterol intake. And even if current intake were assessed accurately, what people eat today may be different than what they were eating years ago. Atherosclerosis is a disease that develops slowly over several decades. In a homogenous population the variation in dietary cholesterol intake varies more from day to day that does average variation between individuals, making it easy to mischaracterize an individual's average cholesterol intake based on short-term dietary assessments. Another confounder is that coronary artery disease (CAD) develops slowly over several decades and it is not uncommon for people to reduce their intake of cholesterol-rich foods after they are told they are at elevated risk for CAD. This may also tend to cause data based on observational evidence to be subject to serious confounding known as reverse causation [see footnote for explanation of reverse causation].So observational data is simply too imprecise and unreliable for definitive conclusions about whether or not a dietary variable like cholesterol intake does or does not increase serum cholesterol levels "appreciably" or influences the long term risk of CVD. Importantly, the Eckel review and the new DGAC's report ignored far more reliable data from controlled clinical trials that have demonstrated that for most people increasing dietary cholesterol does in fact increase total serum cholesterol, LDL-C, and apoB levels. Couple the well-established impact of increased dietary cholesterol causing higher levels of serum apoB-containing lipoprotein cholesterol levels with the strong and consistent evidence linking a higher serum apoB-containing lipoprotein cholesterol with more atherosclerosis and more deaths from CAD and it leaves one wondering why the DGAC made the decision to tell Americans there is no credible scientific basis for putting any limit on cholesterol intake. Why then did the Advisory Committee elect to review data from less reliable observational studies and ignore than better quality data from controlled clinical trials? Perhaps the DGAC's second reference was more convincing?Reference #35. Shin JY, Xun P, Nakamura Y, He K. Egg consumption in relation to risk of cardiovascular disease and diabetes: a systematic review and meta-analysis. Am J Clin Nutr. 2013;98(1):146-59. PMID: 23676423. http://www.ncbi.nlm.nih.gov/pubmed/23676423.Here is what the Shin JY et. al. review reported: "RESULTS: A total of 22 independent cohorts from 16 studies were identified, including participants ranging in number from 1600 to 90,735 and in follow-up time from 5.8 to 20.0 y. Comparison of the highest category (?1 egg/d) of egg consumption with the lowest (<1 egg/wk or never) resulted in a pooled HR (95% CI) of 0.96 (0.88, 1.05) for overall CVD, 0.97 (0.86, 1.09) for ischemic heart disease, 0.93 (0.81, 1.07) for stroke, 0.98 (0.77, 1.24) for ischemic heart disease mortality, 0.92 (0.56, 1.50) for stroke mortality, and 1.42 (1.09, 1.86) for type 2 diabetes. Of the studies conducted in diabetic patients, the pooled HR (95% CI) was 1.69 (1.09, 2.62) for overall CVD.CONCLUSIONS: This meta-analysis suggests that egg consumption is not associated with the risk of CVD and cardiac mortality in the general population. However, egg consumption may be associated with an increased incidence of type 2 diabetes among the general population and CVD comorbidity among diabetic patients." (Dr Shin et.al)So Dr. Shin's review article was also based mainly on observational data with very imprecise determination of dietary cholesterol intake. It is likely the latter that made it difficult to find a direct correlation between egg consumption (and presumably cholesterol consumption) and CAD. Nevertheless, Dr. Shin did report that eating more eggs (and presumably cholesterol) was significantly associated with a 42% greater risk of developing type 2 DM. And in those who developed type 2 DM, Dr. Shin reported they had a 69% greater risk of developing serious CAD in subjects who reported consuming more than one egg a day compared to those who reported consuming less than one egg per week. Again, the data was primarily from observational studies with all the problems such data have due to the imprecise measures of cholesterol intake over time and numerous confounding variables. One likely confounder is that subjects with genetic predisposition to have a higher serum cholesterol level would have been more likely told to reduce their egg and cholesterol intake and/or put on cholesterol-lowering drugs than those without such a genetic predisposition. Could this standard medical practice have largely eliminated a real causal association between eating more eggs (or cholesterol) and a greater risk of CVD? Observational data alone does not establish a causal relationship. For that, one needs well-designed randomized controlled clinical trials. It is very difficult to determine one's egg or cholesterol intake over a long period of time but it is pretty easy to determine one's serum cholesterol level at any given point in time and to determine with some accuracy how many eggs and how much cholesterol someone is currently consuming on a weekly or monthly basis in a randomized controlled clinical trial. Since we know that higher serum cholesterol and especially nonHDL-C levels are associated with more CAD over the long term and we know that increased dietary cholesterol elevates mostly nonHDL-C levels in the blood is it not fair to ask why the DGAC choose to ignore such better-quality data? Why ignore more reliable and precise data and draw conclusions from reviews from observational studies in which the precision of dietary cholesterol assessment is questionable and in which there are known and suspected confounding variables that could easily explain why a real causal association may not have been observed?Do Clinical Trials Show Egg Cholesterol Increases Serum Cholesterol?Reliable data from well-designed controlled clinical trials has consistently shown that increasing dietary cholesterol leads to higher serum cholesterol. Couple that evidence with the proven causal association between higher total serum cholesterol (TC), nonHDL-C, and LDL-C levels with more CAD over time and one has to wonder why the DGAC's report chose to ignore such compelling evidence.Let's take a brief look at some of the most credible evidence from well-designed randomized controlled clinical trials that specifically examined the impact of increasing dietary cholesterol (from eggs) on total serum cholesterol levels and/or other serum lipoprotein fractions such as LDL-C levels. Perhaps the most tightly-controlled clinical trial ever conducted on the impact of dietary cholesterol on serum cholesterol levels was conducted by Dr. Fred Mattson and associates back in 1972. This study demonstrated that increasing dietary cholesterol from zero to 317mg/1000kcal in formula diet fed to incarcerated men (harder to cheat when in jail) increased the average TC by about 25% over six weeks. Looking at the data from Dr. Mattson's study, it is clear that TC levels increased for the first 3 weeks in all 3 groups to which dietary cholesterol was added but remained largely unchanged in the group that continued to consume a nearly identical formula that remained cholesterol-free. There also appears to be no adaption to the higher dietary cholesterol intake over the next 3 weeks as the average serum cholesterol levels for the 3 groups with 106, 212, and 317mg of added cholesterol per 1000kcal of formula remained at those elevated levels for the next 3 weeks of the study. The results of Dr. Mattson's study are shown in Figure 1. below: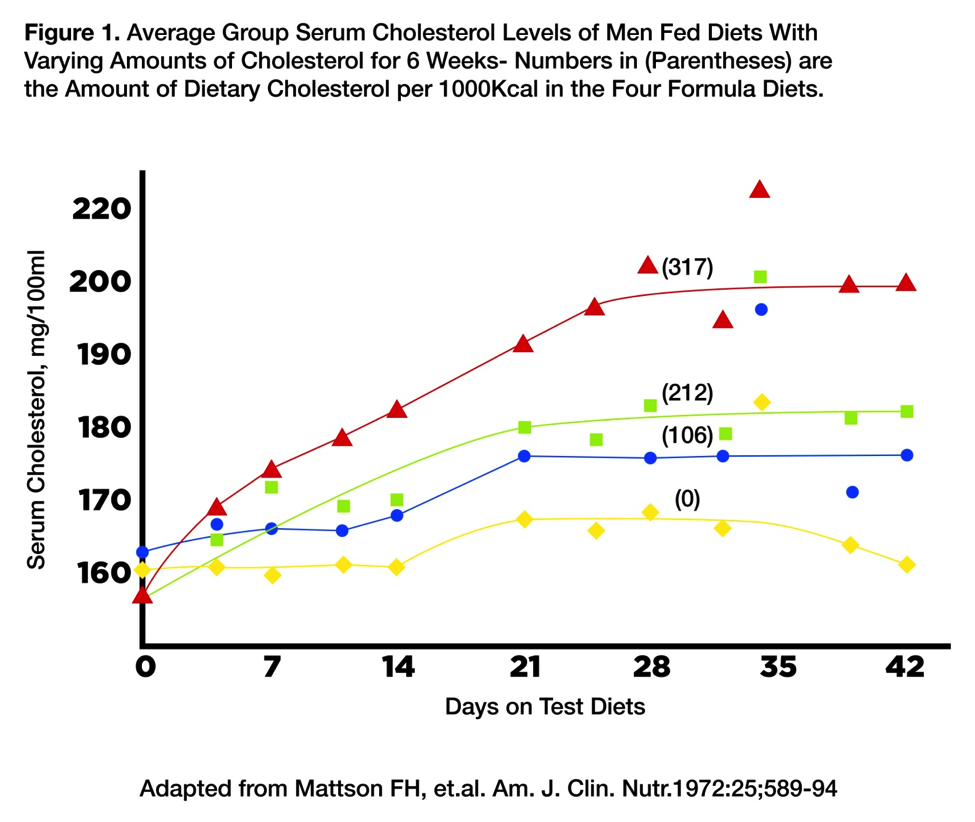 Another study that examined the impact of increasing dietary cholesterol on blood lipids also showed that more eggs and cholesterol elevated the levels of atherogenic apoB-containing lipoproteins in the blood. In this study, Dr. Sacks examined the impact of adding one extra large egg to the diet of a group of 17 lacto-vegetarian college students. The basal diets of these students were quite low in cholesterol because they were avoiding both eggs and meats and consuming only moderate amounts of dairy products. Dr. Sacks at Harvard Medical School reported that when his subjects added one extra large egg a day to their baseline diet for 3 weeks the result was an average increase in their LDL-C level of 12% and an average increase of their apoB level of 9%. Both these increases were statistically significant. Are these not an appreciable increase in LDL-C and apoB levels? The DGAC seems to think these increases would not have an appreciable impact on people's risk of CVD over a lifetime, but that seems to be unwarranted speculation.Of course, those two studies were not funded by the Egg Nutrition Center (ENC) or the American Egg Board (AEB) as were those of other researchers whose trials somehow missed the well-established hypercholesterolemic impact of increasing dietary cholesterol in human subjects. Indeed, it appears some researchers have become adept at designing studies that minimize the well-established hypercholesterolemic impact of increasing dietary cholesterol on serum TC, nonHDL-C, LDL-C, and apoB levels. Sometimes they accomplish this by selecting subjects known to be less responsive to dietary cholesterol changes than average, such as obese, insulin-resistant subjects. They also use free-living subjects whose dietary compliance is not carefully monitored. Poor compliance with dietary instruction in free-living subjects makes it much harder to show real causal associations seen in better-controlled clinical trials. Or they put people on calorie-restricted diets that are known to blunt the hypercholesterolemic impact of both dietary saturated fat and cholesterol during the weight loss phase. Or they vary dietary cholesterol from a high level to a somewhat higher level even though it is known that the impact of dietary cholesterol on serum cholesterol declines with increasing dietary cholesterol intake. This is especially true if all or most of that increased dietary cholesterol occurs at a single meal. It is a sad commentary that with nutrition research it seems increasingly common that those who sponsor that research get what they paid for.So if we focus on the results of studies that were not funded by the egg industry, from carefully-controlled clinical trials with good compliance, those studies generally demonstrate that increasing dietary cholesterol while holding other dietary factors and body weight constant result in significantly increased levels of cholesterol-rich, atherogenic apoB-containing lipoproteins in the blood/serum. So data from controlled clinical trials by researchers with no economic incentive to show eggs don't raise serum cholesterol levels have fairly consistently shown that increasing dietary cholesterol from low levels up to several hundred milligrams per day significantly increases TC, LDL-C, nonHDL-C, and/or apoB levels.Another study that documented the potential dangers of consuming more dietary cholesterol from egg yolks was published in 2012 by scientists at the Stroke Prevention & Atherosclerosis Research Centre in Ontario, Canada. The researchers evaluated the diets of more than 1,200 people (average age 61) who already had CAD. The researchers asked them about their daily diets and about any other CVD risk factors they might have, such as smoking, elevated blood pressure, or diabetes. Then, using carotid ultrasound imaging, the researchers determined the amount of atherosclerosis in their carotid arteries and found a significant correlation between consuming more whole eggs and having more atherosclerotic plaque-ridden arteries. Dr. Spence et. al. noted that the people who had eaten the most eggs over the years had even more plaque build-up in their carotid arteries than did those with the highest cholesterol levels or body weights. His data showed increased dietary cholesterol intake over a lifetime was even more likely to be associated with more atherosclerotic plaque build-up than obesity or even higher serum cholesterol levels.The egg industry must have been concerned about consumer reaction to this new study because immediately after its online publication, doctors affiliated with the industry shot out press statements criticizing the study, pointing out, for example, that the subjects with the higher egg intakes also tended to be heavy smokers. However, these press statements failed to mention that the Canadian scientists had in fact looked for a statistically-significant correlation between egg yolk consumption and smoking history and they found none. Public health ought not be converted into a political battle and biased by economic special interests.Egg Whites vs Whole Eggs StudyAnother carefully-controlled clinical trial conducted by researchers at the University of São Paulo in Brazil fed either three egg whites daily to one group of healthy young men or three whole eggs daily to another group of young, healthy men for 15 days. Except for the variation in egg consumption, both groups of men were consuming the same foods. Their meals were prepared daily by the university and were consistent with the healthier dietary practices being advocated by the DGAC report. The diet was low in saturated fat but high in a variety of whole foods like fruits, green vegetables, beans, chicken, and fish. Dr. Cesar and colleagues reported that among the men in the group eating three egg whites daily, total intake of dietary cholesterol averaged only 174 milligrams per day. By contrast, among the men eating three whole eggs daily, their daily dietary cholesterol intake averaged a whopping 804 milligrams. This large daily increase in dietary cholesterol significantly increased blood cholesterol levels. On average, LDL-C were nearly 40% higher (120 vs 86mg/dl) in subjects consuming 3 whole eggs daily compared to those consuming only 3 egg whites daily. Dr. Cesar concluded that “A high-cholesterol diet clearly enhances LDL-C levels." At the end of the study, the egg white eaters had average LDL levels of only 86mg/dl, while the average LDL-C levels for the group consuming the whole eggs averaged 120mg/dl. Is this the type of change in LDL-C levels the DGAC experts decided was not "appreciable"?As if this marked increase in total-C and LDL-C were not alarming enough, Dr. Cesar and colleagues also reported more troubling news about the impact all that extra dietary cholesterol was having on the postprandial blood lipids of their subjects. In addition to raising fasting LDL-C levels, the subjects consuming the three-whole-eggs-a-day diet also had so much extra cholesterol in their chylomicrons for several hours after eating that it was hindering their liver's ability to efficiently remove the artery-clogging chylomicron remnants from the whole egg eater's blood. Chylomicrons are believed to be another class of atherogenic apoB-containing lipoprotein particles. Chylomicrons are largely responsible for transporting the fat, cholesterol and other fat-soluble dietary components from the gut to the liver and other cells throughout the body. Once chylomicrons have “unloaded” most of their fat (or triglyceride) content, they become cholesterol-rich chylomicron remnants, which are largely cleared from the blood by the liver. However, if these chylomicron remnants are stuffed with more dietary cholesterol, they tend to “hang around” in the bloodstream even longer. These chylomicron remnants, like other apoB-containing lipoproteins in the blood, can enter the artery walls and so also deliver dietary cholesterol to the artery wall just as LDL and remnant VLDL particles do. Therefore, it is almost certain that cholesterol-enriched chylomicron remnants damage the artery wall and promote the growth of atherosclerotic plaques over time. ??It should be noted that these adverse changes to postprandial blood lipids will occur even in people whose fasting blood cholesterol levels are little affected by the increase in dietary cholesterol. This suggests that even in those whose fasting blood lipids seem unaffected by increased dietary cholesterol they may still end up with more atherosclerosis and an increased risk of CAD in response to consuming more dietary cholesterol. Dr. Cesar's study also found that eating three egg yolks daily “increased the residence time of chylomicron remnants, which may have undesirable effects related to the development of coronary artery disease."There is growing evidence that atherosclerosis is caused in part by the postprandial lipemia and this has bolstered concerns about the potentially atherogenic potential of chylomicron-rich remnants. Dr. Anette Varbo examined the association between the developing CAD and variations in blood lipids in 60,608 in Copenhagan. Of those, 10,668 had developed coronary artery disease. Dr. Varbo and colleagues looked for genetic markers that impact various blood lipid levels by genotyping these 60,608 Danes. She found that people who had a genetic predisposition to clear cholesterol-rich remnant lipoproteins more slowly after meals were significantly more likely to develop more inflammation and suffer from more CAD (also called ischemic heart disease - IHD). "Conclusions—Elevated non-fasting remnant cholesterol is causally associated with low-grade inflammation and with IHD, whereas elevated LDL cholesterol is associated causally with IHD without inflammation.”Dr. Varbo and colleagues subsequently published an article reviewing the evidence implicating various lipoprotein particles with risk factors for CAD. They reported "Genetic studies of variants associated with elevated remnant cholesterol levels show that an increment of 1 mmol/L (39 mg/dL) in levels of non-fasting remnant cholesterol associates with a 2.8-fold increased risk of IHD, independently of high-density lipoprotein cholesterol levels. Results from genetic studies also show that elevated levels of remnant cholesterol are causally associated with both low-grade in?ammation and IHD. However, elevated levels of LDL cholesterol are associated with IHD, but not with low-grade in?ammation. Such results indicate that elevated LDL cholesterol levels cause atherosclerosis without a major in?ammatory component, whereas an in?ammatory component of atherosclerosis is driven by elevated remnant cholesterol levels." In the non-fasting state, the remnant lipoprotein particles transporting cholesterol in the blood include both the remnants of VLDL particles produced in the liver and the remnants of chylomicron particles produced by the intestinal mucosa. Diets higher in fat and cholesterol increase the amount of cholesterol in chylomicron particles and so ultimately increase the cholesterol content of chylomicron remnants. Chylomicrons and their remnants, along with VLDL remnants, deliver cholesterol to the artery wall and unlike LDL-C particles do not need to be oxidized before getting picked up by macrophages. Cholesterol-filled macrophages or "foam cells" are largely believed to play a central role in promoting atherosclerotic disease and increasing the release of inflammatory cytokines within the artery wall, increasing the risk of plaque rupture and a heart attack.So if the scientific evidence clearly demonstrates that dietary cholesterol from eggs (or anything else) will increase both fasting and postprandial serum cholesterol levels and higher serum cholesterol levels in apoB-containing lipoproteins are still a well-accepted major risk factor for developing atherosclerosis and increasing the risk of heart disease, then what is it that could be motivating the DGAC Report to recommend dropping any limit on dietary cholesterol from the proposed 2015 US Dietary Guidelines? Could political or economic considerations be a motivating force for this Advisory Committee's recommendation to drop cholesterol from the 2015 USDG?Also ignored by the DGAC were studies like the one by Drs. Shekelle and Stamler. These researchers followed a cohort of 1824 middle-aged men for 25 years. They observed that their intake of dietary cholesterol was significantly associated with an increased risk of death from CAD, from other cardiovascular diseases combined, from all CVD combined, and from all causes combined. They found that relative hazard of death from all CVD combined associated with a higher cholesterol intake was 46% comparing the lowest and top quintiles of dietary cholesterol consumption (an average difference of 184 mg cholesterol/1000 kcal intake). The 46% greater CAD event risk for those the top quintile was after adjustment for age, intake of other dietary lipids, and other coronary risk factors (even including serum cholesterol level). They also found that when they stratified into three groups according to initial serum cholesterol level (those with less than 220 mg/dl, between 220-259 mg/dl, and 260 mg/dl or above), the corresponding relative hazard ratios for those with the top versus bottom quintile of dietary cholesterol intake were 1·58, 1·50, and 1·41, respectively. So the results of the Shakelle & Stamler study showed that increased dietary cholesterol intake was significantly associated with a greater risk of CAD events and this increased risk was partially independent of the increase in serum fasting cholesterol levels. Shekelle & Stamler concluded: "These results are further evidence for the concepts that dietary cholesterol is atherogenic in man, and that the effect is partly independent of serum cholesterol." The results of this study indicate that increased dietary cholesterol appears to be promoting atherosclerosis and increasing the risk of having a heart attack that is partially independent of the effects of that increased dietary cholesterol on fasting serum lipoprotein levels. If dietary cholesterol does indeed promote atherosclerosis in ways that are independent of fasting total-C and LDL-C levels, then it seems likely that increased dietary cholesterol may be doing so at least in part by enriching chylomicron particles with more cholesterol. Couple Drs. Shekelle and Stamler's data with the research of Dr. Varbo and colleagues pointing to the likely atherogenicity of postprandial lipemia and we may have an explanation as to why statin drugs may slow the progression of atherosclerosis but seem less able to reverse CAD than diets very low in fat and cholesterol and high in fiber even when the statins lower fasting LDL-C levels to what appear to be physiologically optimal levels of less than 70-75mg/dl. Since statins do not impact the absorption of cholesterol and fat, they will have little impact on the production of cholesterol-enriched chylomicrons and their remnants. This may be why so many people taking statins still end up with their CAD progressing and why the #1 cause of death in people taking statins is a heart attack.Two Ways Dietary Cholesterol Promotes AtherosclerosisSo there appears to be two different ways in which dietary cholesterol can promote atherosclerosis. One very well-documented way is to increase serum cholesterol levels and mostly apoB containing lipoproteins (nonHDL-C in fasting blood) known to deliver cholesterol artery wall. However, there is growing evidence that dietary cholesterol leads to more cholesterol being absorbed from gut. This increased dietary cholesterol then enriches the cholesterol content of chylomicron particles produced by the intestinal mucosa cells and dumped into the lymphatic system. As we have seen from the data from Drs. Varbo, Shekelle, and Cesar above, there is reason to believe this increases chylomicron cholesterol and alters postprandial blood lipids in ways that promote atherosclerosis that are partially independent of fasting blood lipid levels.The cholesterol-lowering drug Zetia (ezetimbe) is known to work by reducing the absorption of cholesterol from the gut. Plant sterols and tocotrienols also appear to act in a similar way to reduce cholesterol absorption. Reducing cholesterol absorption reduces both postprandial chylomicron cholesterol content and also ends up reducing other apoB-100-containing lipoproteins in fasting blood. Collectively these fasting apoB-containing lipoproteins are nonHDL-C. In effect, one can either reduce cholesterol absorption with drugs like Zetia and resins like cholestyramine or by increasing the dietary intake of plant sterols and tocotrienols and dietary fiber. Alternatively one can reduce cholesterol absorption from the gut simply by consuming less cholesterol-containing foods, with egg yolks being the single largest source of dietary cholesterol for most Americans.So Zetia works to lower plasma levels of total serum cholesterol and LDL-C by inhibiting the activity of the Niemann-Pick C1-like 1 (NPC1L1) protein in the intestinal mucosa cells that enhances the absorption of cholesterol and the excretion of plant sterols. Because this inhibition of NPC1L1 reduces the absorption of dietary cholesterol, it reduces the cholesterol content of chylomicrons and their cholesterol-rich remnants. Human mutations are known to occur that also inactivate a gene encoding for NPC1L1 and so can mimic the action of an inhibitory drug like Zetia (or plant sterols). People who have this genetic mutation can be used to estimate what would happen if the absorption of dietary cholesterol were reduced or enhanced over a lifetime. Dr. Stitzel and colleagues sequenced the exons of NPC1L1 in 7364 patients with coronary heart disease and in 14,728 controls without such disease who were of European, African, or South Asian ancestry. They identified carriers of inactivating mutations (nonsense, splice-site, or frameshift mutations). In addition, they genotyped a specific inactivating mutation (p.Arg406X) in 22,590 patients with CAD and in 68,412 control subjects without evident CAD. They then tested the association between the presence of an inactivating mutation and both plasma lipid levels and the risk of coronary heart disease. They then sequenced their genes and identified 15 distinct NPC1L1 inactivating mutations. They observed 1 of every 650 persons was a heterozygous carrier for 1 of these 15 genetic mutations. Not surprisingly the heterozygous carriers of these NPC1L1 inactivating mutations had a mean LDL-C level that was 12 mg/dl lower on average than that in people who absorbed dietary cholesterol normally because they made normal amounts of NCP1L1 (p<0.05). So the subjects with this genetic mutation were found to have a relative reduction of 53% in the risk of developing CAD. Naturally occurring mutations that disrupt NPC1L1 function were found to be associated with reduced plasma LDL cholesterol levels and a reduced risk of coronary heart disease.What does this data on genetic mutation that impairs the absorption of cholesterol from the gut tell us about the likely impact of absorbing more cholesterol? Well for one thing it suggests that the vast majority of Americans who lack this rare genetic mutation will be absorbing more cholesterol from their gut when they consume more dietary cholesterol. The DGAC was not concerned about this increase in the amount of dietary cholesterol absorbed, claiming that it does not have an "appreciable" effect on LDL-C levels. However, a more troubling question for the DGAC argument is how did a mere 12mg/dl decrease in LDL-C over a lifetime translate into a 53% decreased risk of developing CAD in those who have this NCP1L1 mutation? For the average middle-aged American that 12mg/dl drop in LDL-C would be only about a 6% reduction in LDL-C. Yet long-term clinical trials of lowering LDL-C with high-dose potent statin drugs show reductions in LDL-C of close to 40-60% on average translate into reduced risk CAD deaths of perhaps 30-40%. What could be the plausible mechanism be by which a naturally occurring mutation in NCP1L1 that reduces dietary cholesterol absorption for the gut? Could it be reducing cholesterol absorption from the gut reduces postprandial changes in blood lipids and perhaps other CVD risk factors that are promoting atherosclerosis and CAD in ways that are largely independent of fasting LDL-C levels? Because statin drugs work in the liver to block cholesterol synthesis they have no appreciable impact on NCP1L1 or cholesterol absorption from the gut. If postprandial lipemia plays a major role in the progression of atherosclerosis, then this may explain why statins often slow the progression of atherosclerosis but rarely reverse it. Indeed, one reason why statins may be less effective for reducing the risk of having a heart attack may be because too many patients actually start consuming more cholesterol-rich foods after their MDs tell them their fasting LDL-C look "great." Clearly there is a need for more research on the impact of dietary cholesterol on both fasting and postprandial blood lipids. However, from this reviewer's perspective, it appears Dr. Zilversmit back in 1979 was on to something when he postulated that atherosclerosis may well be largely a postprandial phenomenon.Will 2015 USDG on Cholesterol be a Win for Propaganda, a Loss for Science?The dropping of any limit of dietary cholesterol intake for Americans being recommended by the DGAC (if adopted) will make the 2015 USDG a major victory in the long-standing battle between the American Egg Board (AEB) and nutrition researchers. It will be a loss for those who favor science over dogma and profits. Here's a link that shows some of the AEB's long-running PR efforts to distort and misrepresent the scientific data that clearly shows eating more eggs increases serum cholesterol levels: http://nutritionfacts.org/video/eggs-and-cholesterol-patently-false-and-misleading-claims/However, the new DGAC guidelines will continue to recommend limits on saturated fat and trans fat but no longer for dietary cholesterol. So what is the rationale for limiting saturated fatty acids (SFA) & trans fatty acids (TFA)? Well the main reason to limit these "bad" fats is the research proving increased dietary intake of SFA & TFA increases the levels of TC, LDL-C, nonHDL-C, and apoB in the blood, coupled with data proving that higher levels of these blood lipids promote more atherosclerosis and lead to more coronary artery disease (CAD). So the new guidelines absolutely are not saying Americans no longer need be concerned about elevated levels of atherogenic apoB-containing lipoproteins in the blood, right? The new USDG say limit SFA & TFA largely because they raise nonHDL-C levels and higher nonHDL-C levels are known to promote atherosclerosis and lead to more heart attacks. Can't argue with that logic, right? So the best scientific evidence continues to show that higher TC, LDL-C, nonHDL-C, and apoB levels (whether due to genes and/or diet) promote more atherosclerosis and lead to more heart attacks in the long term. So the DGAC says limit SFA & TFA because they raise the levels of atherogenic apoB-containing lipoproteins in the blood. But the DGAC says that there is no longer any need to limit dietary cholesterol, even though the best quality scientific evidence continues to demonstrate that increasing dietary cholesterol also raises those same atherogenic apoB-containing lipoproteins as do SFA & TFA. Does that make sense?A recent study showed that people who have a genetic variant that increases their LDL-C level about 10% over their entire lives compared to those without that genetic variant have a 50% increased risk of having a heart attack over their lifetime compared with those whose serum cholesterol levels are only 10% lower thanks to their genes. Clearly the best scientific evidence tells us that higher TC, LDL-C, nonHDL-C, and apoB levels (whether due to genes and/or diet) promote atherosclerosis and lead to more heart attacks. Even lowering these apoB-containing lipoproteins with statins and other drugs for a few years significantly reduces the risk of dying from a heart attack, despite the fact that these drugs themselves are not completely innocuous.So while higher nonHDL-C levels are still "bad", the new DGAC's report tells us that more dietary cholesterol is no longer something Americans should try to limit. Does this mean that the scientific evidence now demonstrates all the prior US Dietary Guidelines recommendations to limit dietary cholesterol intake must have been wrong about dietary cholesterol increasing TC, LDL-C, nonHDL-C, and apoB levels? Nope. Does it at least mean that a high intake of dietary cholesterol won't increase your risk of CAD provided your serum cholesterol levels don't increase much or remains low perhaps thanks to taking statins and other drugs? Perhaps not if dietary cholesterol does in fact alter postprandial lipoprotein levels in ways that promote the growth of atherosclerotic plaques and allow them to progress and/or become more inflamed. Sadly for the DGAC committee there is now even more research suggesting that dietary cholesterol alters postprandial lipemia in ways likely to promote atherosclerosis in ways that are at least partially independent of fasting blood lipoprotein levels. Should this evidence have been ignored by the DGAC experts?Why Might the New US Dietary Guidelines Lead to More Atherosclerosis?Perhaps the DGAC dropped a cholesterol limit to better focus on the overall dietary choices than on single substances. After all most foods high in cholesterol are also high in saturated fat, so limiting saturated fat alone would encourage Americans to cut back on fatty meats, cheese, and butter. Why not just simplify the message and tell Americans to cut back saturated fat? Telling people to limit cholesterol intake, they may have figured would happen automatically if they can get Americans to reduce saturated fat, so they may have felt that also telling people to limit dietary cholesterol would have been largely redundant. Of course, we all remember when prior US Dietary Goals/Guidelines experts decided it was too complicated to tell Americans to just avoid saturated fat, so they told them to reduce all fat back in the 1977. The result of those dietary goals was that the commercial food industry started making foods lower in total fat but not necessarily with any improvement in the ratio of omega-6 PUFA to SFA. And when the food industry cut the fat content of many food products, they often increased the sugar, salt, and refined grains. In retrospect those goals should have focused more on SFA and cholesterol and less on the percentage of fat calories. Can we now predict what might go wrong with removing any focus on dietary cholesterol in the 2015 US Dietary Guidelines?Is it possible that by taking away any limit on dietary cholesterol and focusing instead on saturated fat that the American egg industry will start promoting the consumption of eggs by pointing out they are lower in saturated fat than say, salmon? A 7-oz raw piece of salmon contains 6g of saturated fat but only 109mg of cholesterol. By comparison, 3 whole eggs raw contain 4.8g of saturated fat but 561mg of cholesterol. So according to the proposed 2015 USDG, the 3 eggs become the "better" choice than salmon because the eggs have less saturated fat, even though the 3 eggs have more than 5 times the cholesterol content as the salmon and far less omega-3 PUFA. Also, a pound of raw shrimp contains 731mg of cholesterol but still less than 1/2g of saturated fat. If dietary cholesterol is of no concern, then there is really no reason not to consume a lot of shrimp. However, that extra cholesterol from a pound of shrimp would be expected to increase fasting serum cholesterol levels by 10%-15% and likely also alter postprandial blood lipids in ways that would also promote atherosclerosis. And that 10-15% increase in LDL-C would likely be even greater if the pound of shrimp at the "all you can eat" buffet is consumed in place of beans or tofu. Indeed, one cup of tofu has 4X more saturated fat than a pound of raw shrimp or squid. Eating a lot of eggs and shrimp instead of salmon and tofu would not lower the levels of atherogenic lipoproteins in the blood and reduce the risk of CAD but actual increase the risk. However, if one looks only at saturated fat content and ignores dietary cholesterol, what message do the new DGAC experts think might be a plausible result? If Americans stop focusing on dietary cholesterol they may well end eating more squid, shrimp, and eggs but eat less tofu, beans, and salmon. That would be a logical interpretation of the new 2015 US Dietary Guidelines if one accepts the DGAC's seemingly-naïve idea that dropping any limit on dietary cholesterol won't have any "appreciably" bad effects on the health of Americans. We shall see?As we've seen in the past, researchers often underestimate the ability of the commercial food industry to exploit advice that on the surface seems simpler for the public but creates an opening to promote foods that are of questionable value for promoting better health. I'd hate to see history repeat itself based on what, from my perspective, is a naïve position on the likely consequences of their decision to drop any limit on dietary cholesterol. What do you think?Bottom Line:While there is much to like about the DGAC's report, their decision to drop any limit on dietary cholesterol does not appear to be based on the most credible scientific evidence. Why did the DGAC apparently chose to ignore all the data from well-designed controlled clinical trials that have clearly shown greater consumption of dietary cholesterol significantly increases total serum cholesterol, LDL-C, nonHDL-C, and apoB? In the last several years, evidence continues to mount that suggests dietary cholesterol also increases postprandial chylomicron cholesterol levels and there is growing credible evidence that more chylomicron cholesterol also promotes atherosclerosis and CAD independently of elevations of fasting apoB-containing lipoprotein cholesterol levels. Since there is a well-established causal association between increased levels of these atherogenic apoB-containing lipoproteins in the blood with an increased risk of CAD, does it not appear that the DGAC's conclusions about dietary cholesterol no longer being of any concern appear to not be based on the most credible scientific evidence? From this reviewer's perspective, the DGAC's decision to drop any limits on dietary cholesterol intake will result in Americans consuming more dietary cholesterol. That increased dietary cholesterol will promote atherosclerosis and tend to increase the risk of CAD leaving this reviewer to suggest that in the long term the committee members who pushed for this change may well be the ones ending up having egg on their faces.Footnote:Reverse causality refers either to a direction of cause-and-effect contrary to a common presumption or to a two-way causal relationship in, as it were, a loop. So reverse causation can occur when people change their diet after developing a disease or perhaps having a close family member suffer a heart attack. So when lifelong smokers are told they have lung cancer or emphysema, many may then quit smoking. This change of behavior after the disease develops can make it seem like ex-smokers are actually more likely to die of emphysema or lung cancer than current smokers. It is also known that many alcoholics become nondrinkers after being diagnosed with cirrhosis of the liver. Such changes can confuse or confound what is a causal correlation between dying of a disease and an environmental factor. Clearly smokers and alcoholics’ decision to stop smoking or drinking did not cause them to get sick and die. Even so, this tendency to reduce or eliminate things that make you become such after the fact can undermine the statistical correlation between smoking and dying of lung cancer and heavy alcohol consumption and dying of liver disease. When people become concerned about their risk of having a heart attack being high because of family history of heart disease, chest pain, or being told by their MD they are at higher risk, they are more likely than the general population to reduce their intake of foods high in saturated fat and cholesterol. So while these people's current diets may be lower in saturated fat and cholesterol they may still be more likely to have a heart attack. Clearly their cutting back on saturated fat and cholesterol-rich foods did not increase their risk of having a heart attack or heart surgery to open blocked coronary arteries. Nevertheless, statistically these high-risk people may be more likely to have a heart attack or heart surgery despite their now healthier-than-average diets. Observational studies that ask people what they are eating today and then observe who has a heart attack or gets heart surgery over the next few years cannot differentiate between subjects who have an increased risk of such cardiac events despite their recent change of diet. In this case fear of, disease caused them to improve their diet rather than their improved diet caused their cardiac event. So reverse causation occurs when a heightened risk of disease leads people to make diet and/or lifestyle changes in hopes of reducing that risk, but those changes were either too little or came too late. This is one reason observational studies cannot tell us what caused what.References:
Another study that examined the impact of increasing dietary cholesterol on blood lipids also showed that more eggs and cholesterol elevated the levels of atherogenic apoB-containing lipoproteins in the blood. In this study, Dr. Sacks examined the impact of adding one extra large egg to the diet of a group of 17 lacto-vegetarian college students. The basal diets of these students were quite low in cholesterol because they were avoiding both eggs and meats and consuming only moderate amounts of dairy products. Dr. Sacks at Harvard Medical School reported that when his subjects added one extra large egg a day to their baseline diet for 3 weeks the result was an average increase in their LDL-C level of 12% and an average increase of their apoB level of 9%. Both these increases were statistically significant. Are these not an appreciable increase in LDL-C and apoB levels? The DGAC seems to think these increases would not have an appreciable impact on people's risk of CVD over a lifetime, but that seems to be unwarranted speculation.Of course, those two studies were not funded by the Egg Nutrition Center (ENC) or the American Egg Board (AEB) as were those of other researchers whose trials somehow missed the well-established hypercholesterolemic impact of increasing dietary cholesterol in human subjects. Indeed, it appears some researchers have become adept at designing studies that minimize the well-established hypercholesterolemic impact of increasing dietary cholesterol on serum TC, nonHDL-C, LDL-C, and apoB levels. Sometimes they accomplish this by selecting subjects known to be less responsive to dietary cholesterol changes than average, such as obese, insulin-resistant subjects. They also use free-living subjects whose dietary compliance is not carefully monitored. Poor compliance with dietary instruction in free-living subjects makes it much harder to show real causal associations seen in better-controlled clinical trials. Or they put people on calorie-restricted diets that are known to blunt the hypercholesterolemic impact of both dietary saturated fat and cholesterol during the weight loss phase. Or they vary dietary cholesterol from a high level to a somewhat higher level even though it is known that the impact of dietary cholesterol on serum cholesterol declines with increasing dietary cholesterol intake. This is especially true if all or most of that increased dietary cholesterol occurs at a single meal. It is a sad commentary that with nutrition research it seems increasingly common that those who sponsor that research get what they paid for.So if we focus on the results of studies that were not funded by the egg industry, from carefully-controlled clinical trials with good compliance, those studies generally demonstrate that increasing dietary cholesterol while holding other dietary factors and body weight constant result in significantly increased levels of cholesterol-rich, atherogenic apoB-containing lipoproteins in the blood/serum. So data from controlled clinical trials by researchers with no economic incentive to show eggs don't raise serum cholesterol levels have fairly consistently shown that increasing dietary cholesterol from low levels up to several hundred milligrams per day significantly increases TC, LDL-C, nonHDL-C, and/or apoB levels.Another study that documented the potential dangers of consuming more dietary cholesterol from egg yolks was published in 2012 by scientists at the Stroke Prevention & Atherosclerosis Research Centre in Ontario, Canada. The researchers evaluated the diets of more than 1,200 people (average age 61) who already had CAD. The researchers asked them about their daily diets and about any other CVD risk factors they might have, such as smoking, elevated blood pressure, or diabetes. Then, using carotid ultrasound imaging, the researchers determined the amount of atherosclerosis in their carotid arteries and found a significant correlation between consuming more whole eggs and having more atherosclerotic plaque-ridden arteries. Dr. Spence et. al. noted that the people who had eaten the most eggs over the years had even more plaque build-up in their carotid arteries than did those with the highest cholesterol levels or body weights. His data showed increased dietary cholesterol intake over a lifetime was even more likely to be associated with more atherosclerotic plaque build-up than obesity or even higher serum cholesterol levels.The egg industry must have been concerned about consumer reaction to this new study because immediately after its online publication, doctors affiliated with the industry shot out press statements criticizing the study, pointing out, for example, that the subjects with the higher egg intakes also tended to be heavy smokers. However, these press statements failed to mention that the Canadian scientists had in fact looked for a statistically-significant correlation between egg yolk consumption and smoking history and they found none. Public health ought not be converted into a political battle and biased by economic special interests.Egg Whites vs Whole Eggs StudyAnother carefully-controlled clinical trial conducted by researchers at the University of São Paulo in Brazil fed either three egg whites daily to one group of healthy young men or three whole eggs daily to another group of young, healthy men for 15 days. Except for the variation in egg consumption, both groups of men were consuming the same foods. Their meals were prepared daily by the university and were consistent with the healthier dietary practices being advocated by the DGAC report. The diet was low in saturated fat but high in a variety of whole foods like fruits, green vegetables, beans, chicken, and fish. Dr. Cesar and colleagues reported that among the men in the group eating three egg whites daily, total intake of dietary cholesterol averaged only 174 milligrams per day. By contrast, among the men eating three whole eggs daily, their daily dietary cholesterol intake averaged a whopping 804 milligrams. This large daily increase in dietary cholesterol significantly increased blood cholesterol levels. On average, LDL-C were nearly 40% higher (120 vs 86mg/dl) in subjects consuming 3 whole eggs daily compared to those consuming only 3 egg whites daily. Dr. Cesar concluded that “A high-cholesterol diet clearly enhances LDL-C levels." At the end of the study, the egg white eaters had average LDL levels of only 86mg/dl, while the average LDL-C levels for the group consuming the whole eggs averaged 120mg/dl. Is this the type of change in LDL-C levels the DGAC experts decided was not "appreciable"?As if this marked increase in total-C and LDL-C were not alarming enough, Dr. Cesar and colleagues also reported more troubling news about the impact all that extra dietary cholesterol was having on the postprandial blood lipids of their subjects. In addition to raising fasting LDL-C levels, the subjects consuming the three-whole-eggs-a-day diet also had so much extra cholesterol in their chylomicrons for several hours after eating that it was hindering their liver's ability to efficiently remove the artery-clogging chylomicron remnants from the whole egg eater's blood. Chylomicrons are believed to be another class of atherogenic apoB-containing lipoprotein particles. Chylomicrons are largely responsible for transporting the fat, cholesterol and other fat-soluble dietary components from the gut to the liver and other cells throughout the body. Once chylomicrons have “unloaded” most of their fat (or triglyceride) content, they become cholesterol-rich chylomicron remnants, which are largely cleared from the blood by the liver. However, if these chylomicron remnants are stuffed with more dietary cholesterol, they tend to “hang around” in the bloodstream even longer. These chylomicron remnants, like other apoB-containing lipoproteins in the blood, can enter the artery walls and so also deliver dietary cholesterol to the artery wall just as LDL and remnant VLDL particles do. Therefore, it is almost certain that cholesterol-enriched chylomicron remnants damage the artery wall and promote the growth of atherosclerotic plaques over time. ??It should be noted that these adverse changes to postprandial blood lipids will occur even in people whose fasting blood cholesterol levels are little affected by the increase in dietary cholesterol. This suggests that even in those whose fasting blood lipids seem unaffected by increased dietary cholesterol they may still end up with more atherosclerosis and an increased risk of CAD in response to consuming more dietary cholesterol. Dr. Cesar's study also found that eating three egg yolks daily “increased the residence time of chylomicron remnants, which may have undesirable effects related to the development of coronary artery disease."There is growing evidence that atherosclerosis is caused in part by the postprandial lipemia and this has bolstered concerns about the potentially atherogenic potential of chylomicron-rich remnants. Dr. Anette Varbo examined the association between the developing CAD and variations in blood lipids in 60,608 in Copenhagan. Of those, 10,668 had developed coronary artery disease. Dr. Varbo and colleagues looked for genetic markers that impact various blood lipid levels by genotyping these 60,608 Danes. She found that people who had a genetic predisposition to clear cholesterol-rich remnant lipoproteins more slowly after meals were significantly more likely to develop more inflammation and suffer from more CAD (also called ischemic heart disease - IHD). "Conclusions—Elevated non-fasting remnant cholesterol is causally associated with low-grade inflammation and with IHD, whereas elevated LDL cholesterol is associated causally with IHD without inflammation.”Dr. Varbo and colleagues subsequently published an article reviewing the evidence implicating various lipoprotein particles with risk factors for CAD. They reported "Genetic studies of variants associated with elevated remnant cholesterol levels show that an increment of 1 mmol/L (39 mg/dL) in levels of non-fasting remnant cholesterol associates with a 2.8-fold increased risk of IHD, independently of high-density lipoprotein cholesterol levels. Results from genetic studies also show that elevated levels of remnant cholesterol are causally associated with both low-grade in?ammation and IHD. However, elevated levels of LDL cholesterol are associated with IHD, but not with low-grade in?ammation. Such results indicate that elevated LDL cholesterol levels cause atherosclerosis without a major in?ammatory component, whereas an in?ammatory component of atherosclerosis is driven by elevated remnant cholesterol levels." In the non-fasting state, the remnant lipoprotein particles transporting cholesterol in the blood include both the remnants of VLDL particles produced in the liver and the remnants of chylomicron particles produced by the intestinal mucosa. Diets higher in fat and cholesterol increase the amount of cholesterol in chylomicron particles and so ultimately increase the cholesterol content of chylomicron remnants. Chylomicrons and their remnants, along with VLDL remnants, deliver cholesterol to the artery wall and unlike LDL-C particles do not need to be oxidized before getting picked up by macrophages. Cholesterol-filled macrophages or "foam cells" are largely believed to play a central role in promoting atherosclerotic disease and increasing the release of inflammatory cytokines within the artery wall, increasing the risk of plaque rupture and a heart attack.So if the scientific evidence clearly demonstrates that dietary cholesterol from eggs (or anything else) will increase both fasting and postprandial serum cholesterol levels and higher serum cholesterol levels in apoB-containing lipoproteins are still a well-accepted major risk factor for developing atherosclerosis and increasing the risk of heart disease, then what is it that could be motivating the DGAC Report to recommend dropping any limit on dietary cholesterol from the proposed 2015 US Dietary Guidelines? Could political or economic considerations be a motivating force for this Advisory Committee's recommendation to drop cholesterol from the 2015 USDG?Also ignored by the DGAC were studies like the one by Drs. Shekelle and Stamler. These researchers followed a cohort of 1824 middle-aged men for 25 years. They observed that their intake of dietary cholesterol was significantly associated with an increased risk of death from CAD, from other cardiovascular diseases combined, from all CVD combined, and from all causes combined. They found that relative hazard of death from all CVD combined associated with a higher cholesterol intake was 46% comparing the lowest and top quintiles of dietary cholesterol consumption (an average difference of 184 mg cholesterol/1000 kcal intake). The 46% greater CAD event risk for those the top quintile was after adjustment for age, intake of other dietary lipids, and other coronary risk factors (even including serum cholesterol level). They also found that when they stratified into three groups according to initial serum cholesterol level (those with less than 220 mg/dl, between 220-259 mg/dl, and 260 mg/dl or above), the corresponding relative hazard ratios for those with the top versus bottom quintile of dietary cholesterol intake were 1·58, 1·50, and 1·41, respectively. So the results of the Shakelle & Stamler study showed that increased dietary cholesterol intake was significantly associated with a greater risk of CAD events and this increased risk was partially independent of the increase in serum fasting cholesterol levels. Shekelle & Stamler concluded: "These results are further evidence for the concepts that dietary cholesterol is atherogenic in man, and that the effect is partly independent of serum cholesterol." The results of this study indicate that increased dietary cholesterol appears to be promoting atherosclerosis and increasing the risk of having a heart attack that is partially independent of the effects of that increased dietary cholesterol on fasting serum lipoprotein levels. If dietary cholesterol does indeed promote atherosclerosis in ways that are independent of fasting total-C and LDL-C levels, then it seems likely that increased dietary cholesterol may be doing so at least in part by enriching chylomicron particles with more cholesterol. Couple Drs. Shekelle and Stamler's data with the research of Dr. Varbo and colleagues pointing to the likely atherogenicity of postprandial lipemia and we may have an explanation as to why statin drugs may slow the progression of atherosclerosis but seem less able to reverse CAD than diets very low in fat and cholesterol and high in fiber even when the statins lower fasting LDL-C levels to what appear to be physiologically optimal levels of less than 70-75mg/dl. Since statins do not impact the absorption of cholesterol and fat, they will have little impact on the production of cholesterol-enriched chylomicrons and their remnants. This may be why so many people taking statins still end up with their CAD progressing and why the #1 cause of death in people taking statins is a heart attack.Two Ways Dietary Cholesterol Promotes AtherosclerosisSo there appears to be two different ways in which dietary cholesterol can promote atherosclerosis. One very well-documented way is to increase serum cholesterol levels and mostly apoB containing lipoproteins (nonHDL-C in fasting blood) known to deliver cholesterol artery wall. However, there is growing evidence that dietary cholesterol leads to more cholesterol being absorbed from gut. This increased dietary cholesterol then enriches the cholesterol content of chylomicron particles produced by the intestinal mucosa cells and dumped into the lymphatic system. As we have seen from the data from Drs. Varbo, Shekelle, and Cesar above, there is reason to believe this increases chylomicron cholesterol and alters postprandial blood lipids in ways that promote atherosclerosis that are partially independent of fasting blood lipid levels.The cholesterol-lowering drug Zetia (ezetimbe) is known to work by reducing the absorption of cholesterol from the gut. Plant sterols and tocotrienols also appear to act in a similar way to reduce cholesterol absorption. Reducing cholesterol absorption reduces both postprandial chylomicron cholesterol content and also ends up reducing other apoB-100-containing lipoproteins in fasting blood. Collectively these fasting apoB-containing lipoproteins are nonHDL-C. In effect, one can either reduce cholesterol absorption with drugs like Zetia and resins like cholestyramine or by increasing the dietary intake of plant sterols and tocotrienols and dietary fiber. Alternatively one can reduce cholesterol absorption from the gut simply by consuming less cholesterol-containing foods, with egg yolks being the single largest source of dietary cholesterol for most Americans.So Zetia works to lower plasma levels of total serum cholesterol and LDL-C by inhibiting the activity of the Niemann-Pick C1-like 1 (NPC1L1) protein in the intestinal mucosa cells that enhances the absorption of cholesterol and the excretion of plant sterols. Because this inhibition of NPC1L1 reduces the absorption of dietary cholesterol, it reduces the cholesterol content of chylomicrons and their cholesterol-rich remnants. Human mutations are known to occur that also inactivate a gene encoding for NPC1L1 and so can mimic the action of an inhibitory drug like Zetia (or plant sterols). People who have this genetic mutation can be used to estimate what would happen if the absorption of dietary cholesterol were reduced or enhanced over a lifetime. Dr. Stitzel and colleagues sequenced the exons of NPC1L1 in 7364 patients with coronary heart disease and in 14,728 controls without such disease who were of European, African, or South Asian ancestry. They identified carriers of inactivating mutations (nonsense, splice-site, or frameshift mutations). In addition, they genotyped a specific inactivating mutation (p.Arg406X) in 22,590 patients with CAD and in 68,412 control subjects without evident CAD. They then tested the association between the presence of an inactivating mutation and both plasma lipid levels and the risk of coronary heart disease. They then sequenced their genes and identified 15 distinct NPC1L1 inactivating mutations. They observed 1 of every 650 persons was a heterozygous carrier for 1 of these 15 genetic mutations. Not surprisingly the heterozygous carriers of these NPC1L1 inactivating mutations had a mean LDL-C level that was 12 mg/dl lower on average than that in people who absorbed dietary cholesterol normally because they made normal amounts of NCP1L1 (p<0.05). So the subjects with this genetic mutation were found to have a relative reduction of 53% in the risk of developing CAD. Naturally occurring mutations that disrupt NPC1L1 function were found to be associated with reduced plasma LDL cholesterol levels and a reduced risk of coronary heart disease.What does this data on genetic mutation that impairs the absorption of cholesterol from the gut tell us about the likely impact of absorbing more cholesterol? Well for one thing it suggests that the vast majority of Americans who lack this rare genetic mutation will be absorbing more cholesterol from their gut when they consume more dietary cholesterol. The DGAC was not concerned about this increase in the amount of dietary cholesterol absorbed, claiming that it does not have an "appreciable" effect on LDL-C levels. However, a more troubling question for the DGAC argument is how did a mere 12mg/dl decrease in LDL-C over a lifetime translate into a 53% decreased risk of developing CAD in those who have this NCP1L1 mutation? For the average middle-aged American that 12mg/dl drop in LDL-C would be only about a 6% reduction in LDL-C. Yet long-term clinical trials of lowering LDL-C with high-dose potent statin drugs show reductions in LDL-C of close to 40-60% on average translate into reduced risk CAD deaths of perhaps 30-40%. What could be the plausible mechanism be by which a naturally occurring mutation in NCP1L1 that reduces dietary cholesterol absorption for the gut? Could it be reducing cholesterol absorption from the gut reduces postprandial changes in blood lipids and perhaps other CVD risk factors that are promoting atherosclerosis and CAD in ways that are largely independent of fasting LDL-C levels? Because statin drugs work in the liver to block cholesterol synthesis they have no appreciable impact on NCP1L1 or cholesterol absorption from the gut. If postprandial lipemia plays a major role in the progression of atherosclerosis, then this may explain why statins often slow the progression of atherosclerosis but rarely reverse it. Indeed, one reason why statins may be less effective for reducing the risk of having a heart attack may be because too many patients actually start consuming more cholesterol-rich foods after their MDs tell them their fasting LDL-C look "great." Clearly there is a need for more research on the impact of dietary cholesterol on both fasting and postprandial blood lipids. However, from this reviewer's perspective, it appears Dr. Zilversmit back in 1979 was on to something when he postulated that atherosclerosis may well be largely a postprandial phenomenon.Will 2015 USDG on Cholesterol be a Win for Propaganda, a Loss for Science?The dropping of any limit of dietary cholesterol intake for Americans being recommended by the DGAC (if adopted) will make the 2015 USDG a major victory in the long-standing battle between the American Egg Board (AEB) and nutrition researchers. It will be a loss for those who favor science over dogma and profits. Here's a link that shows some of the AEB's long-running PR efforts to distort and misrepresent the scientific data that clearly shows eating more eggs increases serum cholesterol levels: http://nutritionfacts.org/video/eggs-and-cholesterol-patently-false-and-misleading-claims/However, the new DGAC guidelines will continue to recommend limits on saturated fat and trans fat but no longer for dietary cholesterol. So what is the rationale for limiting saturated fatty acids (SFA) & trans fatty acids (TFA)? Well the main reason to limit these "bad" fats is the research proving increased dietary intake of SFA & TFA increases the levels of TC, LDL-C, nonHDL-C, and apoB in the blood, coupled with data proving that higher levels of these blood lipids promote more atherosclerosis and lead to more coronary artery disease (CAD). So the new guidelines absolutely are not saying Americans no longer need be concerned about elevated levels of atherogenic apoB-containing lipoproteins in the blood, right? The new USDG say limit SFA & TFA largely because they raise nonHDL-C levels and higher nonHDL-C levels are known to promote atherosclerosis and lead to more heart attacks. Can't argue with that logic, right? So the best scientific evidence continues to show that higher TC, LDL-C, nonHDL-C, and apoB levels (whether due to genes and/or diet) promote more atherosclerosis and lead to more heart attacks in the long term. So the DGAC says limit SFA & TFA because they raise the levels of atherogenic apoB-containing lipoproteins in the blood. But the DGAC says that there is no longer any need to limit dietary cholesterol, even though the best quality scientific evidence continues to demonstrate that increasing dietary cholesterol also raises those same atherogenic apoB-containing lipoproteins as do SFA & TFA. Does that make sense?A recent study showed that people who have a genetic variant that increases their LDL-C level about 10% over their entire lives compared to those without that genetic variant have a 50% increased risk of having a heart attack over their lifetime compared with those whose serum cholesterol levels are only 10% lower thanks to their genes. Clearly the best scientific evidence tells us that higher TC, LDL-C, nonHDL-C, and apoB levels (whether due to genes and/or diet) promote atherosclerosis and lead to more heart attacks. Even lowering these apoB-containing lipoproteins with statins and other drugs for a few years significantly reduces the risk of dying from a heart attack, despite the fact that these drugs themselves are not completely innocuous.So while higher nonHDL-C levels are still "bad", the new DGAC's report tells us that more dietary cholesterol is no longer something Americans should try to limit. Does this mean that the scientific evidence now demonstrates all the prior US Dietary Guidelines recommendations to limit dietary cholesterol intake must have been wrong about dietary cholesterol increasing TC, LDL-C, nonHDL-C, and apoB levels? Nope. Does it at least mean that a high intake of dietary cholesterol won't increase your risk of CAD provided your serum cholesterol levels don't increase much or remains low perhaps thanks to taking statins and other drugs? Perhaps not if dietary cholesterol does in fact alter postprandial lipoprotein levels in ways that promote the growth of atherosclerotic plaques and allow them to progress and/or become more inflamed. Sadly for the DGAC committee there is now even more research suggesting that dietary cholesterol alters postprandial lipemia in ways likely to promote atherosclerosis in ways that are at least partially independent of fasting blood lipoprotein levels. Should this evidence have been ignored by the DGAC experts?Why Might the New US Dietary Guidelines Lead to More Atherosclerosis?Perhaps the DGAC dropped a cholesterol limit to better focus on the overall dietary choices than on single substances. After all most foods high in cholesterol are also high in saturated fat, so limiting saturated fat alone would encourage Americans to cut back on fatty meats, cheese, and butter. Why not just simplify the message and tell Americans to cut back saturated fat? Telling people to limit cholesterol intake, they may have figured would happen automatically if they can get Americans to reduce saturated fat, so they may have felt that also telling people to limit dietary cholesterol would have been largely redundant. Of course, we all remember when prior US Dietary Goals/Guidelines experts decided it was too complicated to tell Americans to just avoid saturated fat, so they told them to reduce all fat back in the 1977. The result of those dietary goals was that the commercial food industry started making foods lower in total fat but not necessarily with any improvement in the ratio of omega-6 PUFA to SFA. And when the food industry cut the fat content of many food products, they often increased the sugar, salt, and refined grains. In retrospect those goals should have focused more on SFA and cholesterol and less on the percentage of fat calories. Can we now predict what might go wrong with removing any focus on dietary cholesterol in the 2015 US Dietary Guidelines?Is it possible that by taking away any limit on dietary cholesterol and focusing instead on saturated fat that the American egg industry will start promoting the consumption of eggs by pointing out they are lower in saturated fat than say, salmon? A 7-oz raw piece of salmon contains 6g of saturated fat but only 109mg of cholesterol. By comparison, 3 whole eggs raw contain 4.8g of saturated fat but 561mg of cholesterol. So according to the proposed 2015 USDG, the 3 eggs become the "better" choice than salmon because the eggs have less saturated fat, even though the 3 eggs have more than 5 times the cholesterol content as the salmon and far less omega-3 PUFA. Also, a pound of raw shrimp contains 731mg of cholesterol but still less than 1/2g of saturated fat. If dietary cholesterol is of no concern, then there is really no reason not to consume a lot of shrimp. However, that extra cholesterol from a pound of shrimp would be expected to increase fasting serum cholesterol levels by 10%-15% and likely also alter postprandial blood lipids in ways that would also promote atherosclerosis. And that 10-15% increase in LDL-C would likely be even greater if the pound of shrimp at the "all you can eat" buffet is consumed in place of beans or tofu. Indeed, one cup of tofu has 4X more saturated fat than a pound of raw shrimp or squid. Eating a lot of eggs and shrimp instead of salmon and tofu would not lower the levels of atherogenic lipoproteins in the blood and reduce the risk of CAD but actual increase the risk. However, if one looks only at saturated fat content and ignores dietary cholesterol, what message do the new DGAC experts think might be a plausible result? If Americans stop focusing on dietary cholesterol they may well end eating more squid, shrimp, and eggs but eat less tofu, beans, and salmon. That would be a logical interpretation of the new 2015 US Dietary Guidelines if one accepts the DGAC's seemingly-naïve idea that dropping any limit on dietary cholesterol won't have any "appreciably" bad effects on the health of Americans. We shall see?As we've seen in the past, researchers often underestimate the ability of the commercial food industry to exploit advice that on the surface seems simpler for the public but creates an opening to promote foods that are of questionable value for promoting better health. I'd hate to see history repeat itself based on what, from my perspective, is a naïve position on the likely consequences of their decision to drop any limit on dietary cholesterol. What do you think?Bottom Line:While there is much to like about the DGAC's report, their decision to drop any limit on dietary cholesterol does not appear to be based on the most credible scientific evidence. Why did the DGAC apparently chose to ignore all the data from well-designed controlled clinical trials that have clearly shown greater consumption of dietary cholesterol significantly increases total serum cholesterol, LDL-C, nonHDL-C, and apoB? In the last several years, evidence continues to mount that suggests dietary cholesterol also increases postprandial chylomicron cholesterol levels and there is growing credible evidence that more chylomicron cholesterol also promotes atherosclerosis and CAD independently of elevations of fasting apoB-containing lipoprotein cholesterol levels. Since there is a well-established causal association between increased levels of these atherogenic apoB-containing lipoproteins in the blood with an increased risk of CAD, does it not appear that the DGAC's conclusions about dietary cholesterol no longer being of any concern appear to not be based on the most credible scientific evidence? From this reviewer's perspective, the DGAC's decision to drop any limits on dietary cholesterol intake will result in Americans consuming more dietary cholesterol. That increased dietary cholesterol will promote atherosclerosis and tend to increase the risk of CAD leaving this reviewer to suggest that in the long term the committee members who pushed for this change may well be the ones ending up having egg on their faces.Footnote:Reverse causality refers either to a direction of cause-and-effect contrary to a common presumption or to a two-way causal relationship in, as it were, a loop. So reverse causation can occur when people change their diet after developing a disease or perhaps having a close family member suffer a heart attack. So when lifelong smokers are told they have lung cancer or emphysema, many may then quit smoking. This change of behavior after the disease develops can make it seem like ex-smokers are actually more likely to die of emphysema or lung cancer than current smokers. It is also known that many alcoholics become nondrinkers after being diagnosed with cirrhosis of the liver. Such changes can confuse or confound what is a causal correlation between dying of a disease and an environmental factor. Clearly smokers and alcoholics’ decision to stop smoking or drinking did not cause them to get sick and die. Even so, this tendency to reduce or eliminate things that make you become such after the fact can undermine the statistical correlation between smoking and dying of lung cancer and heavy alcohol consumption and dying of liver disease. When people become concerned about their risk of having a heart attack being high because of family history of heart disease, chest pain, or being told by their MD they are at higher risk, they are more likely than the general population to reduce their intake of foods high in saturated fat and cholesterol. So while these people's current diets may be lower in saturated fat and cholesterol they may still be more likely to have a heart attack. Clearly their cutting back on saturated fat and cholesterol-rich foods did not increase their risk of having a heart attack or heart surgery to open blocked coronary arteries. Nevertheless, statistically these high-risk people may be more likely to have a heart attack or heart surgery despite their now healthier-than-average diets. Observational studies that ask people what they are eating today and then observe who has a heart attack or gets heart surgery over the next few years cannot differentiate between subjects who have an increased risk of such cardiac events despite their recent change of diet. In this case fear of, disease caused them to improve their diet rather than their improved diet caused their cardiac event. So reverse causation occurs when a heightened risk of disease leads people to make diet and/or lifestyle changes in hopes of reducing that risk, but those changes were either too little or came too late. This is one reason observational studies cannot tell us what caused what.References:
- http://www.health.gov/dietaryguidelines/2015-scientific-report/PDFs/Scientific-Report-of-the-2015-Dietary-Guidelines-Advisory-Committee.pdf
- Sacks FM et al. Ingestion of egg raises plasma LDL-C in free-living subjects. The Lancet March 24, 1984, page 647-9
- Spence, JD, Jenkins JDA, Davignon J. Egg yolk consumption and carotid plaque. Am J Cardiol. 2012;224:469-73
- Cesar TB, Oliveira, Mesquita CH, Maranhao RC. High cholesterol intake modifies chylomicron metabolism in normolipidemic young men. J Nutr 2006:136;971-6 or http://jn.nutrition.org/content/136/4/971.full.pdf+html
- Varbo A, Benn M, Tybjaerg-Hansen A, et al. Elevated Remnant cholesterol causes both low-grade inflammation and ischemic heart disease, whereas elevated low-density lipoprotein cholesterol causes ischemic heart disease without inflammation. Circulation.2013;128:1298-1309
- Varbo A, Benn M, Nordestgaard BG. Remnant cholesterol as a cause of ischemic heart disease: Evidence, definition, measurement, atherogenicity, high risk patients, and present and future treatment. Pharmacology & Therapeutics. 2014:141:358-67
- Shekelle RB, J Stamler. Dietary Cholesterol and Ischemic Heart Disease. The Lancet 1989:333;1177-1179
- O'Keefe JH, Cordain L, Harris WH, et al. Optimal low-density lipoprotein is 50-70mg/dl: Lower is better and physiologically normal. J Am Coll Cardiol. 2004;43:2142-6
- Van Birgelen C, Hartmann M, Mintz GS, et al. Relation between progression and regression of atherosclerotic left main coronary artery disease and serum cholesterol levels as assessed with serial long-term (>12mos)follow-up intravascular ultrasound. Circulation 2003;108:2757-62
- Stitzel NO, Won HH, Morrison AC, et. al. Inactivating mutations in NPC1L1 and protection from coronary heart disease. N Engl J Med. 2014;371(22):2072-82
- Zilversmit DB. Atherogenesis: a postprandial phemomenon. Circulation. 1979;60:473-85
PS For more information, check out Eggs and Cholesterol: Patently False and Misleading Claims.Why such a long post? Well, we thought it was time to truly get into this topic, and a more extensive article than usual offered that possibility. When we were offering it for feedback, one response really encapsulated what we were thinking. Here's what Tom Rifai, MD, FACP offered, "I think that people should also be given access to your full train of thought document because it is through that in which interested people will really grasp the problem of removing cholesterol as a 'nutrient of concern.' I particularly like you're pushing through the logic of the DGAC which would imply that shrimp would be a better choice than tofu or eating lots of eggs would be better than salmon."