More Salt Promotes Hypertension
Most physicians tend to blame hypertension (HTN) more on genes, stress, and weight gain than on dietary salt intake. This may be because, in their clinical experience, weight loss is generally much more effective for reducing elevated blood pressure (BP) than is advice to reduce dietary salt intake. Physicians also often see large drops in BP when their patients sit quietly and relax before their BP is retaken. And physicians also know most of their HTN patients have family members who also have HTN. Many physicians have been led to believe that only a minority of patients are actually “salt-sensitive.” In their clinical experience, physicians observe that few patients respond to advice to reduce salt or sodium consumption. And then we have the results from observational studies like the PURE studies that find no correlation between salt intake and BP except at the very high end and even suggest low sodium intake is associated with increased mortality. Most medical doctors get very little training in nutrition science in medical school and what they do learn about HTN is that it is best treated with one or more BP medications (meds). Given the limited time that most MDs get to spend with their patients and their limited knowledge of nutrition, many pay little attention to salt or sodium intake. Yet the evidence continues to mount linking excessive salt intake to the development of HTN. Despite this, given their training and clinical experience, it is not surprising HTN is viewed by most physicians as a medical condition best treated with BP meds.Evidence Shows Excessive Salt Intake Causes HTNA recent study on monozygotic (MZ) twins suggests that increased dietary salt intake is by far the greatest contributing factor to the development of HTN. The twins included in the study were age 44 on average, and 63% were women, while 96% were Caucasian. BP was taken as an average of three measurements. This study showed differences in sodium intake between identical twins had a greater impact on BP than did differences in BMI, waist circumference, or waist/hip ratio. However, the study did not address other dietary factors or other parameters that may correlate with sodium intake and also influence blood pressure.Dr. Vidyka Kidambi, from Milwaukee's Medical College of Wisconsin, examined the BP of 88 identical or MZ twin pairs with an average age of 44 from Milwaukee and East Lansing area. Dr. Kidambi’s study focused on the 37 MZ twin pairs in which one MZ twin had a BP that differed by at least 10mm/Hg or more compared to their sibling’s BP. BP was measured with neither MZ twin taking any antihypertensive drugs. In these 37 discordant twin pairs, this variation could not have explained by gene differences, making one twin more or less “salt-sensitive” than their sibling since each twin pair had identical genes. In these discordant twin pairs, the BP averaged 138/85mmHg in the twin with the higher BP, compared to only 121/77mmHg for the MZ twin with the lower BP. Dr. Kidambi looked for factors that might have contributed to an average difference of 17/8mmHg. The team found that, on average, the 37 MZ twins with higher BP consumed more sodium than the twins with the lower BP (3,900 versus 3,261 mg/day, respectively). The twin with the higher BP also tended to have a larger waist circumference (41.3 versus 38.6 inches) and higher BMI. However, even after adjusting for differences in measure of central adiposity and body weight Dr. Kidambi’s results showed increased dietary sodium intake was a significantly greater promoter of elevated BP than was BMI, waist circumference, or weight to height (w/h) ratio. Dr. Kidambi’s study was presented in a poster session at the Hypertension 2018 conference, sponsored jointly by the American Heart Association and the American Society of Hypertension (1).The differences in sodium intake between the 37 discordant twin pairs remained significant and were largely independent of central adiposity, suggesting significant sodium sensitivity in these discordant twin pairs, the researchers concluded. Those consuming 16% less sodium daily than their higher BP twin had a significantly lower BP."I'm not surprised that decreased sodium intake was associated with lower BP," commented Matthew Denker, MD, of the Hospital of University of Pennsylvania. "But I was surprised by the effect size seen -- 17 mm/Hg by my quick calculation. This greatly exceeds the typical numbers quoted," he told MedPage Today.Modestly Lowered Salt Intake Led to Much Lower BPSo why was the difference in BP so much greater for such a modestly lower sodium intake in this study? Most likely because this twin study was not a short-term intervention study like the DASH-Sodium Trial, in which the lower-sodium diet was consumed for only a few weeks. Donald Lloyd-Jones, MD, of Northwestern University in Chicago noted that the twin study’s "interesting design" shows what happens when sodium intake remains lower for many years. It is already known from well-designed but short-term controlled clinical trials such as the DASH-Sodium Trial that reducing sodium from the usual levels seen in US population to only 1500mg/day will lower BP in people with stage 1 and stage 2 HTN. The results from the DASH-Sodium trial (2) are shown in Figure 1. In this study, reducing dietary sodium from about 3400mg/day to only 1500mg daily (or a 1900mg/day reduction in sodium) reduced systolic BP on average by only 6.7mm/Hg for those following a typical American diet. Switching to the DASH diet without reducing sodium reduced SBP by an average of 5.9mmHg. Reducing both sodium by 1900mg daily and switching to the DASH diet combined only reduced SBP by an average of 8.9mmHg. All these drops in SBP are far less than the average 17mm/Hg difference between the discordant MZ twins, even though the twin with the lower BP averaged only 639mg of sodium less per day in Dr. Kidambi’s study.Fig. 1 DASH-Sodium Trial Results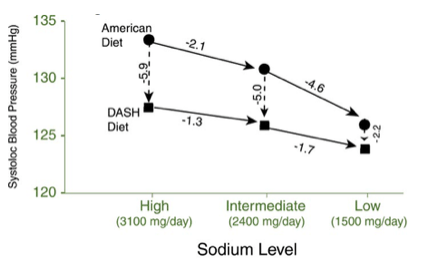 Even the 17mm/Hg difference in SBP observed between these MZ twins is modest compared to the average difference in SBP observed in populations that add very little or no salt to their food compared to those consuming as much or more than the average American. Epidemiological studies have observed that a dietary salt intake of no more than about 30 to 40 mEq (or about 700 to 900 mg of sodium from salt) is associated with a virtual absence of essential HTN (3). Indeed, when comparing human populations that add salt to their food for their whole lives to those who add very little or no salt to their food, the average difference in SBP for people above age 60 is about 50 mmHg (4). The results from the Intersalt study confirm that these large difference in SBP between those consuming a diet with a lot of salt added to populations that add almost no salt to their food appear to result from long-range hypertensive effects from salt toxicity that accrue over the long term via a mechanism that is independent of the short-term hypertensive effects of higher salt intake observed in short-term clinical trials (5).Bottom Line: The results of this study on MZ twins indicates that the impact of too much added salt over the long term is likely far greater than the relatively modest changes in BP observed in short-term clinical trials. However, there is reason to believe that even most of these long-term hypertensive effects of a high salt intake can be largely reversed by adopting a healthful diet low in salt, especially if that low-salt diet is a DASH-style diet and accompanied by exercise and by loss of some excess body weight. Indeed, a study also presented at this recent conference on hypertension suggests that diet and lifestyle changes would likely allow most Americans on BP meds to get off those drugs and control their BP with diet and lifestyle changes alone. More on this study next month.By James J. Kenney, PhD, FACNReferences:
Even the 17mm/Hg difference in SBP observed between these MZ twins is modest compared to the average difference in SBP observed in populations that add very little or no salt to their food compared to those consuming as much or more than the average American. Epidemiological studies have observed that a dietary salt intake of no more than about 30 to 40 mEq (or about 700 to 900 mg of sodium from salt) is associated with a virtual absence of essential HTN (3). Indeed, when comparing human populations that add salt to their food for their whole lives to those who add very little or no salt to their food, the average difference in SBP for people above age 60 is about 50 mmHg (4). The results from the Intersalt study confirm that these large difference in SBP between those consuming a diet with a lot of salt added to populations that add almost no salt to their food appear to result from long-range hypertensive effects from salt toxicity that accrue over the long term via a mechanism that is independent of the short-term hypertensive effects of higher salt intake observed in short-term clinical trials (5).Bottom Line: The results of this study on MZ twins indicates that the impact of too much added salt over the long term is likely far greater than the relatively modest changes in BP observed in short-term clinical trials. However, there is reason to believe that even most of these long-term hypertensive effects of a high salt intake can be largely reversed by adopting a healthful diet low in salt, especially if that low-salt diet is a DASH-style diet and accompanied by exercise and by loss of some excess body weight. Indeed, a study also presented at this recent conference on hypertension suggests that diet and lifestyle changes would likely allow most Americans on BP meds to get off those drugs and control their BP with diet and lifestyle changes alone. More on this study next month.By James J. Kenney, PhD, FACNReferences:
- https://www.abstractsonline.com/pp8/#!/4687/presentation/2908
- Sacks FM, et al. N Engl J Med 2001;344:3-10.
- Houston MC. Sodium and hypertension: a review. Arch Intern Med 1986;146:179-85.
- Joossens JV. Dietary salt restriction, The case in favor. In: Robertson JIS, et al. eds. The therapeutics of hypertension. Congress and Symposium Series, No. 26. Academic Press and the Royal Society of Medicine, 1980;243-50.
- Intersalt Cooperative Research Group. Intersalt: an international study of electrolyte excretion and blood pressure. Results of 24 hour urinary sodium and potassium excretion. Br Med J 1988;297:319-28.